| Home |
| About Us |
| Order |
| Refill |
| Xenical Faq's |
| Dieting |
| Info Articles |
| Contact Us |
|
Calories are Calories Visit your nearest grocery store and on every aisle you will witness one of the most brilliant marketing strategies ever devised. Labels screaming, “Reduced Fat!, Low Fat!, No Fat! And of course Fat Free!” Even fresh squeezed orange juice bottles taut the fat free label in an attempt to boost sales (like a glass of fruit juice ever contained any fat). The sale of low fat products is a thirty billion-dollar industry. Nabisco’s line of Snack Well reduced fat cookies became America’s favorite snack practically overnight. This was the result of Nabisco’s marketing of the low fat label, we know it couldn’t possibly be because of the taste or should we say the aftertaste. The US government has also joined the reduced fat campaign. The Food and Drug Administration now requires virtually all food labels to incorporate the fat content contained in each product, the same label that endorses the thirty-percent of calories from fat recommendation. How has this reduced fat media and marketing attention affected U.S. shopping and eating agendas? A joint survey by The Food Marketing Institute and Prevention Magazine concluded that seventy-two percent of those polled made decisions to purchase concerned with the total fat content of the food product as opposed to the total number of calories presents. What started all of this Reduced Fat, Low Fat, Fat-Free hype? That is anyone’s guess. Statements like “You are what you eat” have been around for decades. Fat probably became the focus of dieting fads because it is the most concentrated source of calories (fat contains nine calories per gram compared to only four calories per gram associated with carbohydrates and proteins). Research also suggests the body prefers to use carbohydrates for fuel while storing fats as fat. According to the Department of Agriculture, individuals are consuming less fat as a percentage of their total caloric consumption. During the mid-nineties fat comprised an estimated thirty-three percent of the caloric intake of U.S. diets compared to forty-percent during the late seventies. So, all this hype must be working? “Americans are consuming significantly less fat as a percentage of their total caloric intake, therefore, as a nation these individuals must be losing weight while enjoying a decrease in the co-morbidity associated with obesity.” NOT THE CASE!!! According to the National Health and Nutrition Examination Survey, the trend in the prevalence of obesity is increasing. The guidelines note that from 1960 to 1997 the prevalence of obesity in adults (BMI) increased from nearly 13 percent to 22.5 percent of the U.S. population; with most of the increase occurring in the 1990’s. How can this increase in obesity be explained? Simply, “Calories are Calories,” while Americans are consuming less fat in their diet they in turn are consuming more calories. The thirty billion dollar a year fat-free food industry combined with their multi-million dollar marketing campaigns have Americans believing fat-free represents calorie-free. So Americans are actually consuming more food, thus, more calories while the fat-free industry laughs their way to the bank. Studies have shown that when individuals are presented with two meals, one believed to be “rich in fat” as compared to “reduced-fat,” individuals will actually consume far less calories eating the meal believed to be “rich in fat.” Individuals tend to, indulge themselves, having second and even third helpings when they believe they are eating “healthy”. Another detail the fat-free industry fails to inform the consumer about is how they are replacing the fat content in their products. Many of the low-fat foods, which have been recently introduced, have simply substituted the fat content with sugars to compensate for the taste lost by the absence of shortening. The problem results from the high caloric content of the sugars added to the fat-free products. So often the low-fat version of foods actually have nearly the same or even more calories than regular product. Reduced fat calorie comparison. During a recent browse through Amazon.com one can only begin to realize just how desperate and/or obsessed the American public actually is with weight reduction. The thought of any of following books actually helping anyone to improve their quality of life over the long term is simply ludicrous. Such titles include: While browsing humorously through more than 150 of the most popular dieting titles, I could not help but notice only two of the authors had a MD following their name. The Doctor’s Walking Diet: How to Lose Weight Without Dieting was not even written by a physician. I am not trying to infer that only those individuals with a higher education are qualified to inform the public. While in medical school, I was afforded the opportunity to work with a gentleman who was fortunate to get an eighth grade education. He had worked for the university for some thirty plus years in the orthopedic research department and was one of the most respected individuals on campus. He was actually the person who instructed all of the medical students how to suture (we learned using pigs feet). Suzanne Somers has spent the last few months on the talk show circuit promoting her new book, Get Skinny Eating Fabulous Foods, I have not wasted my time reviewing this book but I did glance at her previous book Eat Great, Lose Weight Your Fat Is Not Your Fault. This book was inundated with statements, such as, “When you Somersize you can still eat fat and lose weight.” The first 23 pages of her 211 page book has absolutely nothing to do with educating anyone about dieting, she goes on and on giving accolades to her sister in-law for doing all the research for her book. Besides living in the land of opportunity, why? how? do all of these celebrities or ex-celebrities write all of these authoritative books on dieting and health. Please be judicious before starting your next “miracle” diet, the majority of the authors of the current titles have not enrolled in one biochemistry or nutrition class. So how do individuals lose weight and more importantly keep the weight off? First, individuals must understand the concept of diet or dieting. Diet actually comes from the Greek word “dieta,” which means “way of life.” In the situation of obesity, diet is a method of prescribing a new way of living, concentrating on increasing self-esteem while decreasing the prevalence of health complications associated with obesity. Losing and maintaining weight loss in a safe and sensible manner requires a multifaceted approach. Individuals should set realistic and attainable goals develop eating/social behavior patterns that promote success, and incorporate a exercise program designed for the long term. Individuals
must set reasonable and attainable weight reduction goals.
Patients should be aware of their own body-mass-index (BMI). BMI is the most widely used measure of obesity. It is calculated as the weight in kilograms divided by the square of the height in meters (kg/m). This value is independent of age or sex. There are certain limitations to the use of BMI:
Using BMI to measure, national and international health authorities have determined cut-off points to classify normal, overweight and obese individuals
Research has shown as BMI levels increase, average blood pressure and total cholesterol levels increase and average HDL (good cholesterol) levels decrease. Men in the highest obesity category have more than twice the risk of hypertension, high blood cholesterol or both compared to men of normal weight. Women in the highest obesity category have three times the risk of either or both the risk factors. Individuals with a high BMI are also at risk for developing the following diseases:
Individuals should also be advised that waist circumference is an independent prediction of disease risk. A weight circumference of over 40 inches in men and over 35 inches in women signifies increase risk similar to those who have a BMI of 25-39.9. The good news is that even a modest reduction in weight, as little as 5 to 10 percent of your body weight, can significantly improve some life-risk factors. Therefore, all individuals who are overweight should be encouraged to lose even modest amounts of weight to improve their overall health. Individuals should make a zealous effort to continually develop and evolve eating strategies that promote success. There is no book, nor will there ever be a book, that can dictate the precise nutritional regimen each individual should ensue to warrant success. Individuals must devise their own easy to follow eating plan based on moderation, variety and balance. This strategy is the only way the nutritional plan will continue for life. There is no one set plan for any given individual however, these are the facts: To lose weight, fewer calories must be consumed than expended; to maintain weight loss, the number of calories consumed and expended should be approximately equal.
As mentioned repeatedly in this article, consuming reduced-fat, low-fat and fat-free products is not enough to succeed in losing and maintaining weight loss. Individuals must be very conscientious concerning their daily consumption of calories. Education is key, individuals should learn how to eat foods that are naturally low in fat (foods that have not been processed, replacing the fat with high caloric sugars). The more foods are processed, equates to the increased fiber and bulk that have been excised, thus, the more calories per gram. For, example it is now three in the afternoon, the satiety from lunch has long since faded and it is time for a snack. The individual reaches into the refrigerator and snags a twelve-ounce bottle of advertised “fat-free” apple juice and within ten seconds the juice is gone but the appetite still lingers. This individual has just consumed some 165 calories (of his/her allotted 2,000 calories for the day). This glass of juice could have been substituted with a glass of water (zero calories) and an apple (65 calories). The individual would then have enjoyed the satiating effect while the digestive system processed the apple. Snacking between meals is probably the most detrimental aspect to any diet; the key to success is to find snack foods that are palatable, high in bulk/fiber, and low in calories. Back to the apple, when is the last time you sat down and snacked on say two or three apples at one sitting? However, you could sit down and easily consume 10-15 reduced-fat Oreo cookies with a glass of milk comprising some 950 calories or almost half of an individuals daily allotment of calories. The difference is the apple is more filling secondary to the bulk and fiber as compared to cookies with their high sugar content and subsequent high-density calories. Individuals must also learn how to be prepared so they do not set themselves up for failure. Individuals should always have a nutritious low calorie snack available. Do not expect to find something appropriate to eat in a vending machine or at the convenient store around the corner because you will inevitably end up with a bag of Doritos and a Coke. The consumption of alcohol represents another hurdle for many individuals. Alcoholic beverages are full of “empty calories.” Twelve ounces of beer contain approximately 150 calories; the same quantity of light beer contains 105 calories. A glass of wine or shot of 80 proof distilled alcohol contains around 100 calories. If a person were to only consume one beer or one glass of wine over the course of the evening their diet strategy would probably stay intact. However, this is rarely the case, alcohol decreases your inhibitions so once you have consumed one drink it usually results in another. After a couple of drinks an individual’s will power decreases and they will often indulge in poor eating habits. I am not suggesting giving up drinking completely, that would be an unrealistic goal. However, each individual should develop techniques to reduce their alcoholic intake. For example, if a person’s occupation requires them to entertain individuals several times per week, first have a nutritious light meal prior to arriving at the function. Next, make your drink of choice a glass of water with a slice of lemon. Arriving at the function on a semi-full stomach and refraining from alcohol will assist tremendously in keeping an individual’s will power in check. An exercise program is the foundation behind any commitment to improve one’s health. According to the American Heart Association, a 200-pound individual who consumes the same amount of calories but walks briskly each day for 1-2 miles will lose approximately 14 pounds per year. The following chart reveals the number of calories utilized per hour for various activities involving 100, 150 and 200 pound individuals.
Source: American Heart Association Realistically, the calories an individual burns while walking his/her 1-2 miles is probably negated with the refreshing glass of Gatorade consumed upon the completion of the walk. However, the commitment this individual made to drag his/her body out of the warm bed at sunrise to subject oneself to pain, will set a positive atmosphere for the entire day. First, this individual’s metabolism will be in relative shock racing to keep up with an energy expenditure that is usually not reached until way in the late afternoon if reached at all. Secondly, this individual is now developing a sense of self-worth and devotion towards his/her goals. Donuts, sitting in the lobby at work, no longer represent the same temptation nor will second helpings or late-night deserts. Thought processes, such as, “Why should I negate all my early morning workouts by consuming these unhealthy, fattening foods?” begin to dictate actions in a positive manner. Unfortunately, dropout rates from all fitness programs is excessive, statistics indicate that only 20 percent of those individuals that begin an exercise continue to exercise for one year. Exercise programs should be tailored to an individual interests and considerations. For example, ex-basketball players should research where there are pick up games are being played, if golf is your passion, briskly walk the course instead of riding in the cart, ex-swimmers find a masters program that meets at lunch, house-wives start a walking social group, etc. Goals for physical activity should involve a minimum of 20 to 30 minutes 4-5 times per week. Individuals should strive to reach a heart rate that is 60-80 percent of their maximum rate (estimated maximum heart rate can be calculated by using the standard 220 minus an individual’s current age). Individuals, who are creative in developing an exercise agenda, combining physically challenging events in a social atmosphere, are more likely to sustain their efforts over the long term. Research indicates that individuals who include physical activity in their weight loss programs are more likely to succeed in keeping the weight off. In addition to promoting weight control, exercise improves strength and flexibility, increases HDL levels (good cholesterol), reduces individual’s risk of heart disease, and helps to control blood pressure and diabetes, while promoting an overall sense of well being. No review of dieting would be complete without discussing the current pharmacological options available. First of all, there are no “magic pills” that are going to solve the dieting dilemma. The use of appetite suppressants may help individuals over the short term, however, they are not a substitute for developing healthy eating habits over the long term. Therefor use of pharmacotherapy for weight reduction should not commence without an adjunctive diet, behavioral modifications and an exercise program. The Weight Loss Practice Survey, sponsored by the FDA and The National Heart, Lung and Blood Institute, found that 5 percent of women and 2 percent of men trying to lose weight use diet pills. The majority of these diet pills are over-the-counter (OTC) medications, containing the active ingredient phenylpropanolamine (PPA), such as, Dexatrim and Acutrim. “ Using diet pills containing PPA will not make a big difference in the rate of weight loss, even the best studies show only about a half pound or greater weight loss, per week, using OTC pills, combined with diet and exercise,” states, Robert Sherman of the FDA’s Office of OTC Drug Evaluation. The problem with these medications is although they suppress an individual’s appetite early in treatment the medication’s effects are usually short lived. After approximately six weeks or less most individuals become acclimated to the medication and the appetite suppression qualities are minimized. Prescription medications for weight reduction suffered a setback recently when the popular drug combination fenfluramine/phentermine (fen/phen) was linked to valvular heart disease. Prior reports have also linked pulmonary hypertension (increased blood pressure in the lungs) to the treatment with fenfluramine or phentermine alone. Valvular heart disease occurs when a heart valve is compromised so the valve cannot open or close properly. This subsequently effects the flow of blood through the vessels of the heart. Pulmonary hypertension is a rare lung disorder in which the blood pressure in the pulmonary artery increases above normal values. This increased pressure results in an increased strain on the right ventricle of the heart. Some 45 percent of individuals die within four years after acquiring this disorder. Currently, there are several prescription medications used for the treatment or management of obesity. These medications include:
Amphetamines, such as, Dexedrine are no longer in vogue for weight reduction therapy. Most physicians have stopped prescribing amphetamines secondary to their high abuse potential and the risk of individuals becoming psycho-physically dependent on these medications. Sympathomimetic Amines, such as, phentermine hydrochloride continue to be commonly prescribed for weight loss. Although there are concerns about the widespread and indiscriminate use of the medications, most physicians concur the potential for abuse and dependency are mild as compared to the amphetamines. Phentermine is an anorectic medication (decrease an individual’s appetite) with pharmacologic activity similar to the amphetamines. Clinical trials suggest that adult obese individuals, instructed in dietary management and treated with phentermine, lose more weight than those treated with a placebo and diet. The amount of weight loss varies from trial to trial and appears to be associated variables other than the medication. Physician-investigators, the population treated and the diet prescribed all seemed to have an impact on the amount of weight reduction. However, the extent of weight loss of an individual taking phentermine is only a fraction of a pound more than those individuals treated with a placebo. Phentermine is indicated in the treatment of obesity as a short- term adjunct to diet modification and an exercise program. Side affects
associated with phentermine include: Contraindications of to the use of Phentermine include: advanced ateriosclerosis, symptomatic cardiovascular disease, moderate to severe hypertension, hyperthyroidism, known hypersensitivity or idiosyncrasy to the sympathomimetic amines, glaucoma, agitated states, patients with a history of drug abuse, during or within 14 days following the administration of monoamine oxidase inhibitors, (MAO), etc. Neurotransmitter re-uptake inhibitors, such as Meridia (sibutramine hydrochloride monohydrate) generates a therapeutic affect by inhibiting the re-uptake of norepinephrine, serotonine and dopamine in the synaptic cleft of the brain. This subsequently results in an increase in these neurotransmitters; an increase in serotonine produces the early sensation of feeling “full.” Re-uptake inhibitors are not true appetite suppressants. Individuals continue to have the desire to eat but they feel full or content earlier, therefore, they eat less. In clinical trials, individuals treated with Meridia while on a reduced caloric diet, showed a significant weight reduction. In one twelve month study, the average weight loss in patients taking 10mg of sibutamine daily, was approximately 10 lbs. Those individuals taking 15mg daily averaged 14 lbs. in the same time frame. The average weight loss in individuals who were treated with diet alone lost only an average of 3.5 lbs. Conversely, of those individuals on a given dose of Meridia who did not lose at least 4 lbs. in the first four weeks of therapy, approximately 80 percent of those individuals did not go on to achieve significant weight loss. 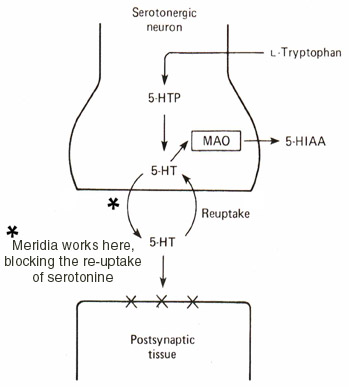 Side affects
associated with Meridia include: Contraindications to the use of Meridia include: those receiving monoamine oxidase inhibitors (MAO’s) or other centrally acting appetite suppressants, patients with a history of coronary artery disease, congestive heart failure, arrhythmias, stroke, anorexic nervosa, uncontrolable hypertension, severe renal impairment, severe hepatic dysfunction, glaucoma, patients with known hypersensitivity to sibutamine or any of the active ingredients in Meridia, etc. Meridia is a controlled substance, schedule IV, physicians should evaluate patients for a history of drug abuse and follow these patients closely, observing them for signs of abuse (tolerance, incremental doses, drug seeking behavior, etc.). Lipase inhibitor, Xenical (orlistat) is a new weight control medication recently approved by the FDA. Distinct from other medications that effect neurotransmitters to stimulate the brain to suppress appetite. Xenical uses a fat blocking mode of action that works non-systemically in the gastrointestinal tract. Dietary fats are large molecules that must be broken down by enzymes, called lipases, before they can be absorbed into the bloodstream. Xenical interferes with these lipases by forming covalent bonds with the them in the stomach and small intestine, this essentially inactivates the enzymes so they are no longer available to hydrolyze dietary fat into an absorbable state. Thus, allowing for some 30 percent of dietary fats to pass through the gastrointestinal tract unchanged. 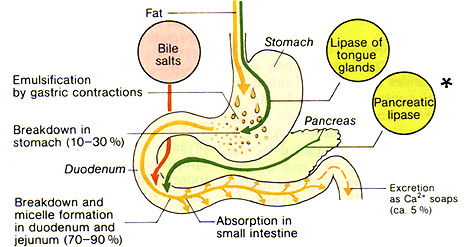 *Xenical® works here, covalently bondings to the pancreatic lipases Clinical studies indicate, in the first year, that individuals treated with Xenical (120 mg per dose, three times per day) and a low calorie diet lost approximately two-thirds more weight than those treated with the same diet and a placebo. In the second year, individuals treated with Xenical and a weight maintenance diet were two times as likely to keep the weight off as individuals on the same diet and a placebo. “This study demonstrates that partial inhibition of fat absorption in obese subjects can produce sustained weight loss,” the authors conclude. “Subjects treated with Orlistat plus a mildly controlled-energy diet lost significantly more weight than those treated with placebo plus diet even though all subjects received a high standard of care and similar dietary counseling… These observations collectively suggest Orlistat may be a useful adjunct to dietary intervention in producing and maintaining weight loss over two years.” Journal of the American Medical Association (JAMA. 1999;281:235-245) Side effects
associated with Xenical include: Contraindications to the use of Xenical include: chronic malabsorption syndromes, cholestasis, individuals with known hypersensitivity to orlistat or any of the active ingredients in Xenical. Two new medications may hold promise for weight reduction in the future: Cholecystokinin is a neurotransmitter in the brain that produces the feeling of satiety. If a medication can increase the effect of this naturally occurring brain chemical, individuals would feel full quicker and presumably eat less. Several pharmaceutical companies are investigating cholecystokinin-boosting agents, however, this potential medication is in the early trials so FDA approval is a few years away. Leptin, is another neurotransmitter known to suppress appetite. Currently, biotechnology is capable of producing the equivalent of the neurotransmitters in mass quantities. Early studies have shown mild weight loss associated with the medication. However, FFD approval is at least a year or more in the future. Of all the above listed medications, Xenical should prove to be the most beneficial and effective medication in the long-term treatment of obesity. Xenical’s ability to block the digestion of some 30 percent of dietary fats represents a significant decrease in the caloric intake for some individuals. Since Xenical works non-systemically in the gastrointestinal tract side effects are minimal. In fact, in therapeutic studies some 97 percent of orlistat was found to be excreted into the feces. This is reassuring, especially following the recent side effects associated with fen/phen (valvular heart disease, pulmonary hypertension). Additionally, with Xenical there are no complications involving tolerance or dependency as the case with the anorectic medications. Therefore, Xenical may be prescribed safely for longer periods of time. ORDER YOUR XENICAL ONLINE NOW! Hopefully the above paragraphs have provoked the reader’s innate common sense so he/she will come to the immediate conclusion that no article, book, medication or marketing agenda is going to immediately cure their lifetime of poor eating habits. Think how long it has taken for most individuals to develop their unhealthy behavior patterns. These routines are not going to be erased by turning the pages in some ex-celebrity’s diet book or popping “miracle” diet pills. CHALLENGE YOURSELF RIGHT NOW TO DEVELOP A NEW WAY OF LIFE!!! Incorporate reasonable and obtainable weight reduction goals, develop and evolve healthy eating strategies, while initiating an exercise program. Remember that even a modest reduction in weight, 5 to10 percent of body weight, can significantly improve many life risk factors. Are you going to be around to see your grandchildren? |
|
Dieting |